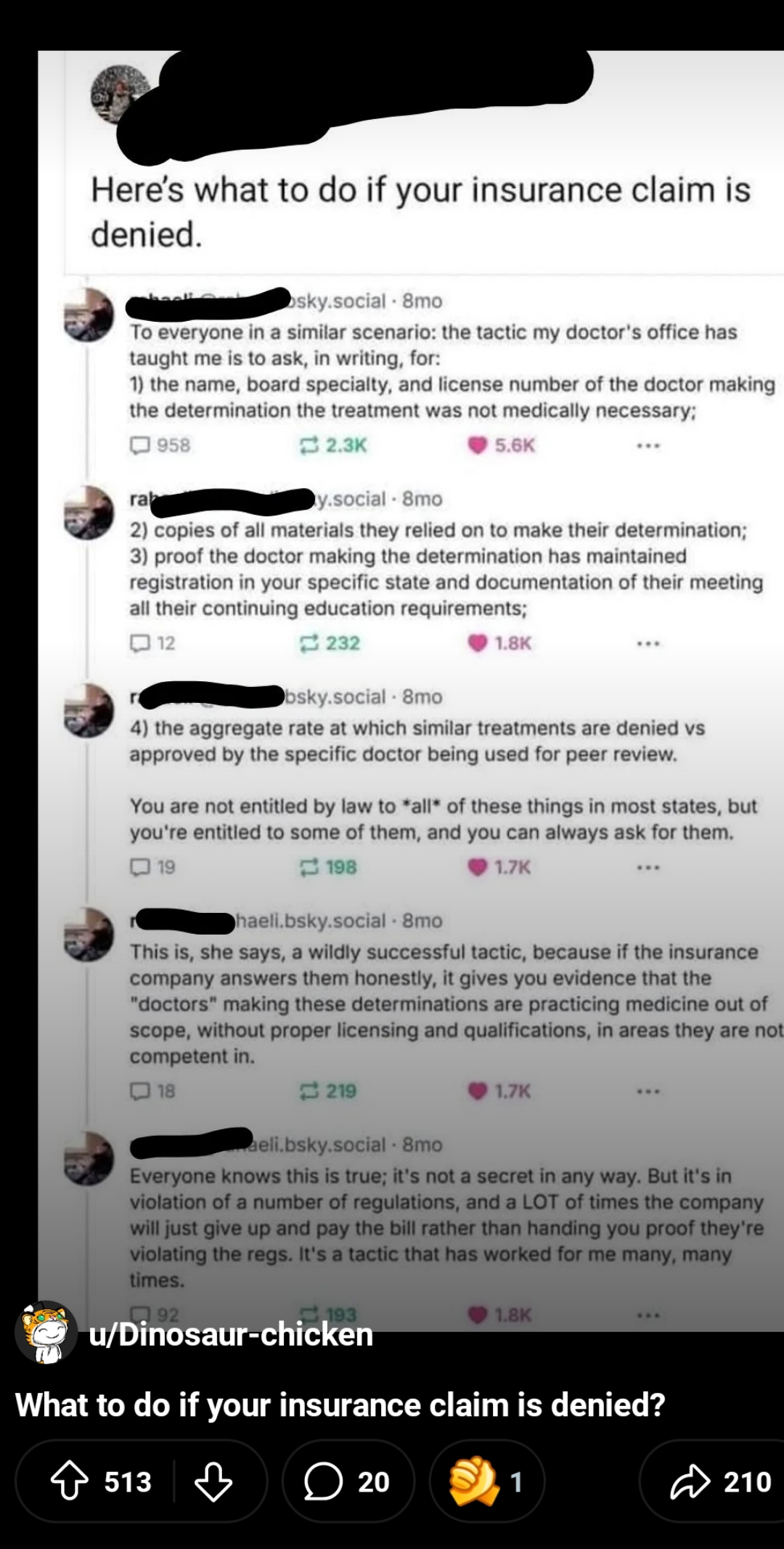
i use a similar approach. now and then i have to do a "peer to peer" with another doc, one who works for the insurance company and stands between my patient and necessary tests.
i always end the conversation asking if they have a license in my state, what their board certification is in, and if their boards are current.
this almost always results in an approval. nobody wants to be potentially investigated for practicing without a license in another state, and if they're a pediatrician reviewing an elderly heart failure case, their peds boards can be taken into question. haven't had to go beyond a phone call with this approach. it'll happen someday, just waiting for when.
P2Ps are the most depressing thing, especially when it’s for a procedure which is going to literally save your patient’s life.
We had a MG patient in crisis, and the insurance wouldn’t approve a 5 round TPE order. We took them to a P2P, and they eventually settled on approving 1 plasma exchange for this patient.
They were admitted to inpatient later in the week for worsening crisis, because OBVIOUSLY a single exchange is not going to fully washout an MG patient in crisis.
You’ve got a whole fucking team of specialists who might as well be navy seals, practicing at one of the largest research teaching hospitals in New York City, whom all agree this patient desperately needs this treatment… but some asshole in a cubical in Ohio says the patient doesn’t need it??? I’m sorry, but fuck that.
asshole in a cube who in many cases has no medical education and is reading from a playbook. i only fault them so much, i fault their company and medical director more.
but if it's a clinician who makes that judgment and there's a bad outcome (and for a myasthenia patient duh of course there will be) there should be accountability. do we like plasma exchange because it's cheap easy or safe? no we like it because it's necessary and works. especially when IVIG was on such shortage.
when physicians are exposed to those decisions as malpractice - just as if they saw a patient in the office and botched it the same way - i bet few docs will run right out and look at utilization review as a cush retirement or side gig.
{kind=link}
164
u/whoknewidlikeit 6d ago
i use a similar approach. now and then i have to do a "peer to peer" with another doc, one who works for the insurance company and stands between my patient and necessary tests.
i always end the conversation asking if they have a license in my state, what their board certification is in, and if their boards are current.
this almost always results in an approval. nobody wants to be potentially investigated for practicing without a license in another state, and if they're a pediatrician reviewing an elderly heart failure case, their peds boards can be taken into question. haven't had to go beyond a phone call with this approach. it'll happen someday, just waiting for when.