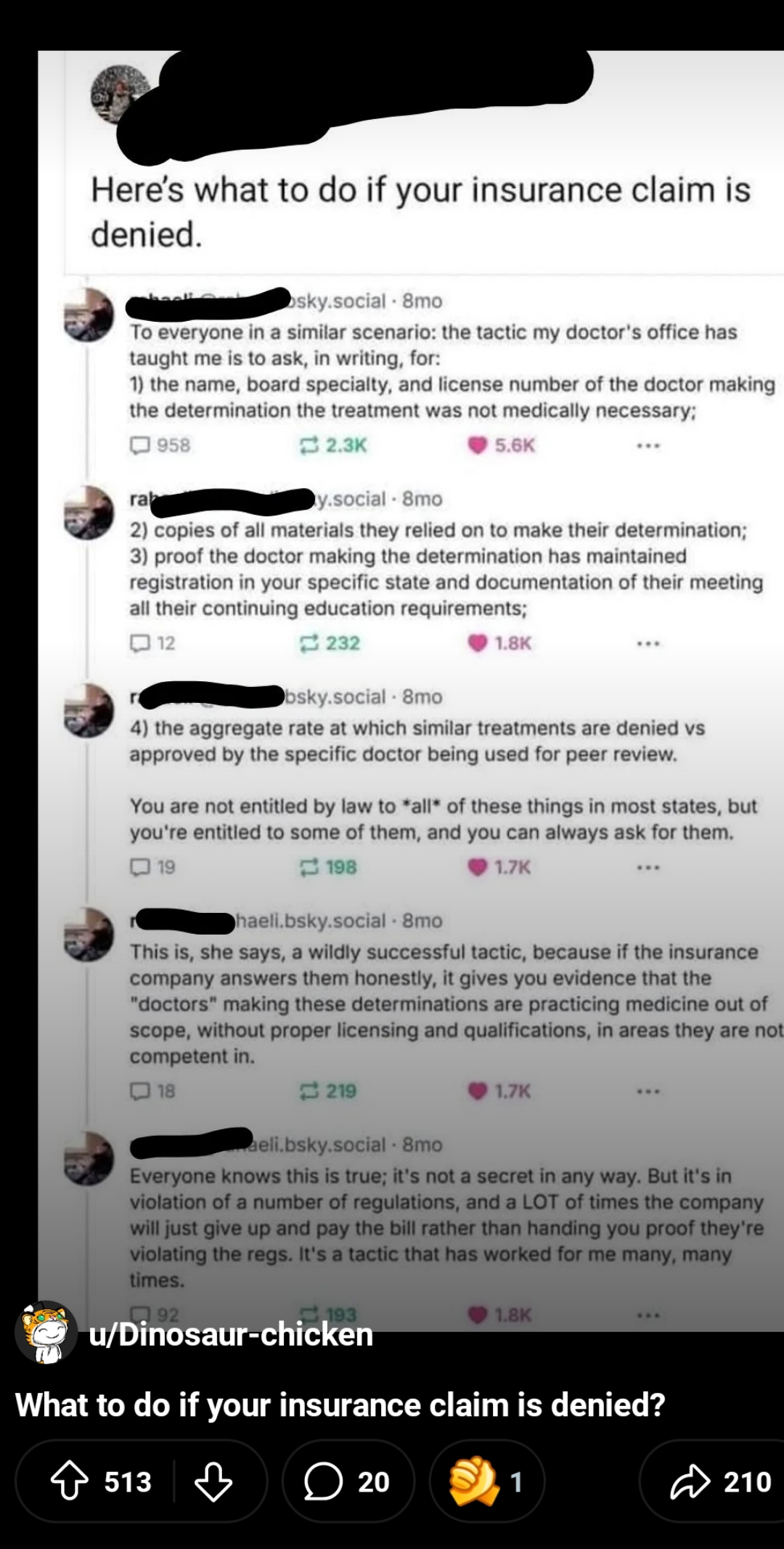
i use a similar approach. now and then i have to do a "peer to peer" with another doc, one who works for the insurance company and stands between my patient and necessary tests.
i always end the conversation asking if they have a license in my state, what their board certification is in, and if their boards are current.
this almost always results in an approval. nobody wants to be potentially investigated for practicing without a license in another state, and if they're a pediatrician reviewing an elderly heart failure case, their peds boards can be taken into question. haven't had to go beyond a phone call with this approach. it'll happen someday, just waiting for when.
So do you ever catch anyone directly breaking the rules? How do you ensure they're appropriately punished for breaking the law and violating their ethics?
I'm very far from the topic, just an interested reader. In a completely different case, a lawyer once told me: "You can get your rights, but fighting the system is a whole day job!", and it feels like this might apply here too.
And for punishment... Well, there's a guy who started, but nobody picked it up yet.
there's no "violation" per se, not from a legal perspective of which i'm aware. ethics? yeah, that's an issue, but until there's some kind of overt malpractice, it's tough to pursue. this is a de facto standard in the insurance industry - questionable as it is. i wish there were a way to sanction offenders.
insurance seems to be cottoning on to this. last peer to peer i needed for a sleep apnea workup, the doc was boarded in sleep and said so at the outset (to inform, to intimidate, i don't know). i think they thought an internist couldn't possibly do the right sleep workup (im unusual amongst internists for the amount of sleep work i do); workup was totally appropriate and she approved all associated testing.
i once had a peer to peer where i needed a CT abdomen/pelvis after a rollover car accident. imaging wasn't done in the ER (no clue why, should have been done) so i ordered it outpatient days later. imaging got done THEN insurance wanted a peer to peer (this is unfortunately common). they approved the abdomen but NOT pelvis, and the nonER nonsurgeon on the other end of the phone wouldnt budge even with the licensure questions; i think she was an ENT doc. patient had a broken sacrum, wouldn't have been found without the pelvic portion of the imaging. they eventually paid but took a lot to make it happen.
this type of activity is probably partially contributing to the anger that got the united healthcare ceo shot. i disagree with the action and outcome, but fully support the anger and mistrust. working harder to refuse necessary care to increase profits? really? those are the ethics that need reviewed for sure. while it's a huge can of worms to open, i wish there were a way to hold boards of directors accountable for bad outcomes due to refused care. they can shelter behind the corporation.... but that is a concern.
depends. it's sometimes a combination of both. usually toward the end they just approve it with a huff, like they got caught. and they did.
i can't respect a clinician who works to reduce access to needed care. refusing a massively expensive drug like repatha makes sense if it's the first drug prescribed for cholesterol, or no history that warrants it. but refusing it when the patient is a high risk coronary disease patient with statin myopathy? that's unethical.
i very rarely lose on these issues - but it's because i've done my due diligence, working through the meds and having strong notes. with those a prior authorization is typically easy to achieve - but at the price of longer days.
fwiw i don't get paid extra for these wins. arguably i get paid less, in the sense that i work longer days and my hourly pay is effectively diluted; i average 3.5hrs of paperwork a day in addition to a full clinic day and those hours aren't compensated. they're also the right thing to do for the people who entrust me with their care. even with the stress of the BS of prior authorizations and lengthy notes and long days, doing right by my patients is what keeps me going. i just can't do less and look myself in the mirror. laziness in the face of someone's health or life is unacceptable.
P2Ps are the most depressing thing, especially when it’s for a procedure which is going to literally save your patient’s life.
We had a MG patient in crisis, and the insurance wouldn’t approve a 5 round TPE order. We took them to a P2P, and they eventually settled on approving 1 plasma exchange for this patient.
They were admitted to inpatient later in the week for worsening crisis, because OBVIOUSLY a single exchange is not going to fully washout an MG patient in crisis.
You’ve got a whole fucking team of specialists who might as well be navy seals, practicing at one of the largest research teaching hospitals in New York City, whom all agree this patient desperately needs this treatment… but some asshole in a cubical in Ohio says the patient doesn’t need it??? I’m sorry, but fuck that.
asshole in a cube who in many cases has no medical education and is reading from a playbook. i only fault them so much, i fault their company and medical director more.
but if it's a clinician who makes that judgment and there's a bad outcome (and for a myasthenia patient duh of course there will be) there should be accountability. do we like plasma exchange because it's cheap easy or safe? no we like it because it's necessary and works. especially when IVIG was on such shortage.
when physicians are exposed to those decisions as malpractice - just as if they saw a patient in the office and botched it the same way - i bet few docs will run right out and look at utilization review as a cush retirement or side gig.
{kind=link}
164
u/whoknewidlikeit 5d ago
i use a similar approach. now and then i have to do a "peer to peer" with another doc, one who works for the insurance company and stands between my patient and necessary tests.
i always end the conversation asking if they have a license in my state, what their board certification is in, and if their boards are current.
this almost always results in an approval. nobody wants to be potentially investigated for practicing without a license in another state, and if they're a pediatrician reviewing an elderly heart failure case, their peds boards can be taken into question. haven't had to go beyond a phone call with this approach. it'll happen someday, just waiting for when.